
From the 1Department of Research, Sunnaas Rehabilitation Hospital, 2Institute of Clinical Medicine, Faculty of Medicine, 3Department of Psychology, University of Oslo, 4Department of Anesthesiology, Oslo University Hospital, 5Norwegian Centre for Violence and Traumatic Stress Studies, University of Oslo, 6Division of Mental Health and Addiction, Oslo University Hospital and 7Department of Behavioral Sciences in Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
Objective: To describe the clinical characteristics and physical functioning in persons hospitalized after 2 terror attacks in Norway in 2011.
Design: Cross-sectional study with retrospective acute medical data.
Subjects: Surviving persons hospitalized with physical injuries.
Methods: Medical and psychological assessments 3–4 years after injury, with data on injury type and severity collected from medical records.
Results: A total of 30 out of 43 potential subjects participated (19 women, 11 men; age range 17–71 years (median 23 years)). Eighteen participants had suffered a severe injury, with New Injury Severity Scale (NISS) scores > 15. All body parts were affected. The number of surgical procedures ranged from 0 to 22 (median 3), and days in intensive care ranged from 0 to 59 (median 2.5), of which 16 had more than 24 h intensive care. Three to 4 years later, a majority of the participants had a broad spectrum of somatic and psychological problems and reduced physical functioning. Two-thirds of the participants reported their physical health to be unsatisfactory, and continuous need for healthcare and unmet needs were identified for all except 4 of the participants.
Conclusion: Persons hospitalized following a terror attack experience a broad spectrum of somatic and psychological problems and need long-term physical and psychological follow-up. This study indicates specific needs for rehabilitation after injuries acquired under psychological traumatic circumstances.
Key words: terrorism; multiple trauma; health status; rehabilitation.
Accepted Jan 15, 2019; Epub ahead of print Feb 27, 2019
J Rehabil Med 2019; 51: 226–234
Correspondence address: Grethe Månum, Sunnaas Rehabilitation Hospital, Bjørnemyrvn. 11, 1450 Nesoddtangen, Norway. E-mail: grethe.manum@sunnaas.no
Victims of terror are at major risk of long-term post-traumatic stress disorder (PTSD) and physical sequelae. Prior research after terrorist attacks has focused primarily on PTSD and the need for mental health services, where being injured has been seen as an indicator of high exposure to the traumatic event and a predictor of the level of psychological distress, rather than as a risk factor for function and healthcare needs. Similar to survivors of natural disasters, the impairments after terror attacks vary in severity, and might include spinal cord injuries, traumatic brain injury, limb amputation, fractures, soft-tissue injuries, and psychological sequelae. This study investigated the medical characteristics, physical functioning, and life satisfaction of people hospitalized with physical injuries due to the 2011 Norway terror events approximately 3 years after the attacks. The assessments revealed a broad spectrum of somatic and psychological problems, reduced physical functioning, and a continuous need for healthcare.
Terror attacks can result in loss of life and large numbers of severely injured persons (1–6). Prior research after terrorist attacks has focused primarily on post-traumatic stress disorder (PTSD) and other mental health issues and, correspondingly, the need for mental health services (7–10). To our knowledge, few studies have addressed long-term somatic health characteristics and physical functioning in physically injured terror victims.
On 22 July 2011, an extremist attacked the Governmental Quarter in Oslo and a youth organization’s summer camp on Utøya Island, Norway, killing 77 people and severely injuring many others (1–3). Previous studies on the injured survivors have focused on their acute medical treatment (2, 3). Many victims underwent multiple surgeries; 18 patients underwent 194 surgical procedures (3). The fragmenting bullets resulted in progressive necrosis and destruction of soft tissue with the risk of sepsis (3). These patients exhibited repetitive debridement; tissue loss was among the primary challenges in the acute phase, and 2 patients were amputated at the elbow or ex-articulated at the shoulder and hip, respectively (3).
The Norwegian Centre for Violence and Traumatic Stress has conducted a longitudinal survey investigating health problems and healthcare needs of the terror victims (e.g. 10–13). These authors found that only somatic symptoms were associated with mental health service utilization when adjusting for psychological symptom level (10), proposing that the somatic symptoms result from somatization. Stene et al. investigated the Utøya attack survivors’ healthcare needs, experiences, and satisfaction with post-terror healthcare 2.5 years after the attack (11). Among the 261 participants (52% of the survivors), 51% (n = 133) a large benefit of healthcare, while 17% (n = 45) reported little or no benefit. Also, 20% (n = 53) reported unmet needs for treatment of psychological reactions. Twenty one percent (n = 56) experienced a need for help with physical health issues, while half (n = 21) of the 43 individuals who reported having significant need for help due to attack-related physical health problems had been physically injured during the attack. The studies regarding PTSD and somatization have suggested that physical injuries and pain worsen the burden of psychological symptoms (12, 13).
Based on the available literature, being injured has been construed as an indicator of high exposure to the traumatic event and a predictor of the level of psychological distress, rather than a risk factor for func-tional limitations and healthcare needs. Likewise, the terror literature is relatively less focused on physical disability and its implication for overall functioning. Similar to natural disasters (14–16), impairments after terror attacks vary in severity, and might include spinal cord injuries, traumatic brain injuries, limb amputation, fractures, soft-tissue injuries, and psychological sequelae (e.g. PTSD, alterations in lifestyle, changes in self-concept, and decreased quality of life).
None of the publications regarding the 2011 Norwegian terror victims have presented long-term findings from comprehensive clinical examinations paired with acute medical data, nor has long-term physical function and health satisfaction in this particular sub-sample of terror victims been investigated.
The main aim of this study was to describe the medical characteristics, physical functioning and life satisfaction of people hospitalized with physical injuries due to the 2011 Norway terror events 3–4 years after the attacks. Based on these assessments, a secondary aim was to identify the current physical and/or psychological healthcare needs of the terror victims.
This cross-sectional study includes retrospective acute medical data from Oslo University Hospital Ullevål (OUHU) trauma register and medical records. The study was approved by the Regional Committee for Medical and Health Research Ethics, Norway. Letters with informed consent forms were delivered by post, including one reminder letter. Non-responders were contacted by telephone. All participants provided written informed consent.
Hospital records at the OUHU regional trauma centre for the South-Eastern Health Region in Norway and Vestre Viken local hospitals were used to identify those who had spent at least 1 night in hospital.
Data collection was performed at Sunnaas Rehabilitation Hospital in Norway between May 2014 and March 2015 (3–4 years post-injury). Acute trauma scores were checked for validity against the OUHU trauma registry. The participants underwent a structured clinical interview, medical examination, psychological assessment, neuropsychological screening, and several standardized questionnaires and assessment methods were applied.
Three experienced medical doctors and 3 rehabilitation psychologists extracted data from medical records, clinical examinations, and interviews, using consistent techniques and standardized procedures developed and adjusted in joint training sessions and consensus processes. The results were presented to and discussed with the participants. A clinical consideration of the participants’ healthcare needs and whether needs were met at the time of assessment was conducted. Clinical discharge summaries were sent to participants and their general practitioners (GPs). Referrals to healthcare services were made, if needed.
Injury characteristics. The Abbreviated Injury Scale (AIS) (17) was used to describe the anatomical injuries. The AIS ranks injuries from 1 to 6 (6 is not survivable). The New Injury Severity Score (NISS), which is the sum of the squares of the 3 highest AIS scores regardless of body region affected, was used to describe the injury severity, classified as minor–moderate (1–8), serious (9–15) or severe–critical (16–75) (18). The acute Glasgow Coma Scale (GCS) (19), number of days in the intensive care unit (ICU), number of surgical procedures, amputations, length of stay in acute hospital, and place of discharge were also registered.
Clinical characteristics. A clinical examination, including neurological, musculoskeletal, and internal organ status was performed. The skin was inspected for presence (yes/no) of scars related to the terror events, and self-perceived burden of injury-related scars was evaluated on a 0–10 numerical rating scale (NRS) (20). A score of 4 or more was used as a cut-off for scar-related distress (20).
The participant’s post-traumatic stress (PTS) symptoms in the preceding month were measured using the University of California at Los Angeles PTSD Reaction Index (21). The total score comprises 17 items that correspond to the 17 DSM-IV symptoms of PTSD, rated on a 5-point Likert scale (range 0 = never; 4 = most of the time). Total scores and numbers of participants with clinical levels of PTS symptoms (cut-off value ≥ 38) are presented (22). Pain impact was measured on a 0–10 NRS assessing the mean pain severity over the previous week (23). A score of 3 or more was used as a cut-off for clinically significant pain (24).
A neuropsychological screening was performed. The California Verbal Learning Test (CVLT-II) (25) and the WAIS-IV digit span tests (26) were included, together with performance-based measures of learning, memory, and attention. Subjective perception of impaired memory and attention was reported on 2 items from the Rivermead Post Concussion Symptoms Questionnaire (27). The participants were asked to compare with premorbid level (i.e. before the terror attacks) and rate the extent of symptoms related to concentration and memory on a scale from 0 to 4 (0 = no problem at all; 4 = severe problem), where scores of ≥ 3 were considered clinically significant (28). The Glasgow Outcome Scale-Extended (GOS-E) was used to assess gross outcome in participants with radiologically verified brain injury (29).
Physical function. The generic Short Form Health Survey (SF-36) physical function scale (PF) was used to assess physical abilities, mobility, and self-care (30). The PF consists of 10 items focused on the extent to which a respondent’s health has limited performance of various physical activities over the past 4 weeks. Responses are provided on a 3-point scale; “yes, limited a lot”, “yes, limited a little”, and “no, not limited at all”. Scores on the individual items were converted into a 0–100 scale (31), with PF total scores below 86.4 being considered to indicate physical limitations (30).
The Barthel ADL index, with a score ranging from 0 to 20, was used to assess independence in daily life (32). Total scores below 4 were considered to indicate dependency in activities of daily living (ADL) (32).
Health characteristics were assessed via a custom-made questionnaire addressing past (before 22 July 2011) and current health problems. The questionnaire assessed the participants’ health status considering current and previous diagnosis and/or treatments of eye/ear conditions, cardiovascular or lung diseases, diabetes mellitus, skin conditions, cancer, rheumatologically or other musculoskeletal conditions (e.g. fibromyalgia), and neurological conditions, including headache as well as gastrointestinal and allergic conditions.
Life satisfaction. The Life Satisfaction Scale (LSS) measures both global and domain-specific life satisfaction and has been well-validated in Sweden, which has a comparable culture to Norway (33, 34). Two items addressing the level of satisfaction with physical and psychological health were included. Items are scored on a 6-point scale, from 1 (very dissatisfied) to 6 (very satisfied). Total scores and dichotomized scores (1–4 (not satisfied) vs 5–6 (satisfied)) are presented (33).
Healthcare. A questionnaire was developed based on that of another research group studying the same terror attacks (10, 11), which included questions regarding previous and current provision of health services (care or treatment), along with their perceived usefulness.
Descriptive statistics were used to describe the study sample. Relations between continuous variables were examined using Spearman’s two-tailed correlation coefficients. Differences between participants above and below the clinical cut-off values were investigated using Mann–Whitney non-parametric 2-sample tests and simple cross-tabulations with Fisher’s exact test. Values of p < 0.05 were considered statistically significant. All analyses were conducted using SPSS v.22 (IBM Corporation, Armonk, NY, USA).
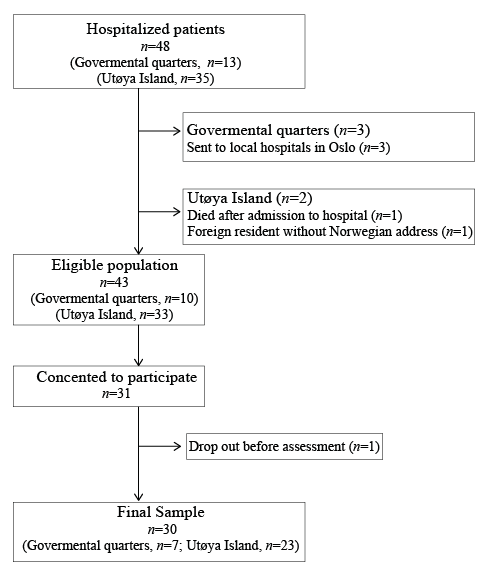
Forty-eight persons were identified as potential participants. As shown in the flow diagram (Fig. 1), 35 were injured at Utøya Island, and 13 in the Governmental Quarter. Of these, 3 persons triaged to local hospitals in Oslo were not contacted (as we did not have access to their identities and assumed their injuries to be minimal, since they would otherwise have been triaged to OUHU) and 2 persons were excluded. A potential sample of 43 persons was thus established, of which 31 were injured at Utøya Island and 10 in the Governmental Quarter. A final sample of 30 persons was included, corresponding to a 70% response rate.
Fig 1. Flow diagram of study participants.
The length of acute hospital stays ranged from 1 to 81 days with a median [Q1, Q3] of 15 days [1, 27]. Five participants were transferred to local hospitals within 30 h, and we do not have access to their total length of hospital stay. The median of 15 might therefore be somewhat too low. If these 5 are not included, the median [Q1, Q3] of 19 days [2, 28]. The participants were discharged to their homes (n = 10), local hospitals (n = 11) or specialized inpatient rehabilitation centres (n = 9). Those transferred to rehabilitation had multiple traumas without central nervous involvement (n = 4) or multiple traumas with traumatic brain injury or spinal cord injury (n = 5).
Table I presents sociodemographic and injury characteristics. Nineteen participants were female. At the time of assessment, the median age was 23 years. The age range was 19–71 years, and only 5 individuals were older than 30 years. Twenty-one persons lived by themselves, and 9 with their parents. All but 5 participants were engaged in work or education between 50% and full-time.
Table I. Socio-demographics, injury severity and acute hospital care of the participants
As shown in Table I, the primary mechanisms of trauma were gunshots and explosion forces. Eighteen participants were initially classified as having a severe injury with NISS-scores above 15. The number of days in the ICU and the number of surgical procedures reflect large variation in both injury severity and complications. Three participants did not undergo surgery, and 5 had 10 or more procedures, with 22 surgeries at the most. The physical injuries were heterogeneous and ranged from contusions to multiple life-threatening internal organ and central nervous system injuries. As shown in Fig. 2, there were injuries in all body regions, and as many as 23 sustained injuries to more than 1 body region. A total of 15 participants sustained their principal injury to their head, neck, spinal cord, thorax or abdomen; according to the AIS scores shown in Fig. 2, these subjects suffered life-threatening injuries. Four of the participants had brain injuries verified by computed tomography (CT) scans. Two of these had GCS scores of 5 and 8, respectively, indicating severe brain injury. Several participants had gunshot injuries to internal organs (kidney, heart, lung, and gastrointestinal tract). More than two-thirds (n = 22, 73.3%) had injuries to their extremities, and 12 had extremity injuries as their primary injury. More than half of the participants (n = 17, 56.7%) had major injuries to their skin and subcutaneous tissues, but only 2 had this type of injury as their only injury. Extremity injuries resulted in 4 amputations in the subacute phase. All of these were scored as AIS = 3, by definition the most severe level of extremity injury.
Fig. 2. Body region of most severe injury and distribution of additional injuries according to the Abbreviated Injury Scale (AIS).
As shown in Table II, most participants had several sequelae due to their initial injuries. Ten participants had visual, cognitive, motor or sensory impairments caused by injuries to their central or peripheral nervous system. Four had amputations that included a finger, an arm, a leg, or both an arm and a leg, respectively. Nine participants had prominent soft-tissue defects (e.g. shoulder, arm, abdominal or lower limb muscles). Trauma-related reduction of muscle strength and joint range of motion were found in 6 and 3 participants, respectively. All except one had skin injury from the trauma and/or surgical procedures, manifesting as scars that were accompanied by varying degrees of complaints. Sixteen reported no complaints related to their scars, while 10 of the participants reported distress at a level of 4 or higher, along with a preference to cover up their scars.
Table II. Clinical characteristics 3 years after the terror attacks
As shown in Table II, the median [Q1, Q3 ] PTSD-RI and pain values were 15 [7.8, 29.0] and 6.5 [3.3, 7.8] , respectively. Four participants were scored as having clinical levels of PTS symptoms. Twenty-five participants reported having pain in the week before assessment, and 12 were considered to have clinically significant pain (NRS pain > 3).
Two of the 4 participants with a brain injury scored 5 and 6 on the GOS-E, indicating moderate disability. For the 26 participants with no brain injury, the normal results on tests of memory and attention were in contrast to subjective experience of reduced concentration and memory (Table II). Exploratory analyses revealed no statistically significant correlation between subjective cognitive complaints and test-performance on CVLT-II or WAIS-IV Digit-span. However, significant correlations were found with current pain levels as well as symptoms of post-traumatic stress (r range, 0.45–0.74, all p < 0.02).
Most participants (n = 23) reported health problems, and 7 reported more than one health problem. Twenty persons had sustained injuries to the body area in which they reported health problems. Examples of these problems were gastrointestinal disorders (e.g. abdominal pain and flatulence), skin conditions (e.g. dysaesthesia, itching and pain from the areas with soft-tissue defects and/or scars), reduced lung capacity, tinnitus, and neurological deficits already reported. Fourteen participants reported health problems before the terror event, but only 2 reported more than one health problem.
Three participants had a Barthel ADL Index score below 4, reflecting the need for help in ADL. Thirteen participants presented a reduced SF-36 PF mean score (<86.4) (30). Two-thirds specified limitations in vigorous activities (e.g. running or heavy lifting), and one-third limitations in lifting or carrying groceries or climbing several flights of stairs. No statistical significant correlations were detected between the SF-36 PF and NISS (r = –0.306, p = 0.30) or SF-36 PF and PTSD-RI (r = – 0.326, p = 0.079), but significant correlations were found between SF-36 PF and pain (r = –0.61, p < 0.001).
All participants had received healthcare follow-up since being discharged from the hospital. As shown in Table III, follow-up conducted by a GP or psychologist/psychiatrist was the most common, both after hospital discharge and at the time of study inclusion. While 9 participants were referred to specialized inpatient rehabilitation in the early phase, only 2 received regular rehabilitation services at the time of study inclusion. Of the initial 6 participants receiving regular healthcare provision from pain specialists, only 4 were receiving specialized pain treatment at study inclusion.
Table III. Healthcare provision since discharge from somatic hospital
Healthcare needs were identified for all but 4 participants (Table IV). Thus, the evaluation of clinical findings with current care provision indicated somatic and/or psychological health issues in most of the participants, several of whom had more than 1 health condition.
Table IV. Healthcare needs
The participants presented symptoms and/or clinical findings that resulted in referral for a radiological examination (e.g. bony prominences), or a visit to an ear, nose and throat specialist (e.g. weak or hoarse voice), plastic surgeon (reconstructive surgery for scars), orthopedic surgeon (e.g. knee issues), pain specialist or GP. Clinical recommendations to the GP were, for example, related to vocational benefits (n = 2), oral medication (n = 5) and management/follow-up of hypertension (n = 2). Ten participants presenting with complex pain condition were discussed with or reffered to a pain specialist.
For 4 participants who did not benefit adequately from ongoing psychological treatment, we either contributed to strengthening the ongoing treatment, or provided additional follow-up with another expert.
Eighteen participants were in need of rehabilitation. Of these, 11 already received adequate help, and 7 were referred to multidisciplinary rehabilitation (n = 2) or physiotherapy (n = 5). Examples of clinical recommendations in these referrals included evaluation of orthopaedic aids and goal-oriented training to increase functional ability.
Twenty-two participants reported their physical health to be unsatisfactory, and 17 reported their psychological health to be unsatisfactory (Table II). Of the 22 participants reporting unsatisfactory physical health, 15 also reported unsatisfactory psychological health. Thus, 2 participants were unsatisfied only with their psychological health while 7 reported unsatisfactory physical health, but satisfactory psychological health. Six participants reported both their physical and psychological health to be satisfactory. Only 2 participants reported satisfactory physical health and unsatisfactory psychological health.
When comparing the 15 participants reporting both their psychological and physical health to be unsatisfactory with those reporting combinations of satisfactory physical or psychological health, we found no statistical significant differences in NISS scores, but significantly worse SF-36 PF-, pain- and PTSD-RI total scores in the group reporting unsatisfactory physical and psychological health (data not shown). The same results were found when comparing participants reporting their physical health as being unsatisfactory (n = 22), with participants reporting their physical health as being satisfactory (n = 8) (Table V). Significant correlations were found between scores of physical or psychological health and SF-36 PF (r = 0.58, p < 0.001 and r = 0.42, p = 0.021, respectively).
Table V. Study participant’s satisfaction with physical health
Ongoing healthcare needs were identified in all 15 participants reporting their psychological and physical health to be unsatisfactory. Of these, 13 were referred further, while 2 had already been referred by their GP.
This study describes the long-term clinical characteristics of those hospitalized with physical injuries after the 2011 terror attacks in Oslo. The assessments revealed a broad spectrum of somatic and psychological problems, reduced physical functioning, and a continuous need for healthcare. More than two-thirds of the study participants (n = 22) reported their physical health to be unsatisfactory, and only 6 reported both their physical and psychological health to be satisfactory 3–4 years after the terrorist attacks. Taken together, the findings shed light on the particular mechanism at play in persons who acquire physical injuries under extreme psychological conditions, and also indicate long-term rehabilitation needs in this group.
Previous publications pertaining the same terror events have described the injury severity of hospitalized survivors (2, 3). Our assessments indicate that the injuries caused by the terror events represented a causal factor for most of the study participants’ long-term somatic complaints and reduced physical functioning. The clinical investigations revealed that neurological deficits causing paresis or neuropathic pain, amputations, gastrointestinal disorders, tinnitus, and skin complaints were in accordance with the injury sites. However, more non-specific complaints, such as dizziness and headache, were also identified; supporting the knowledge that emotional symptoms may predispose for somatic symptoms (12, 13, 35). Our results are in accordance with the studies by Stene et al. (10) and Bugge et al. (13) on the Utøya survivors, stating that somatic symptoms could be related directly to the physical injuries.
As this study investigated those hospitalized with physical injuries, reduced physical functioning was expected. The failure to detect significant correlations between physical functioning and injury severity, but significant correlation with pain, is noteworthy. The non-significant correlation between NISS and physical function seems reasonable, since the initial NISS score did not reflect the clinical findings of later amputations, peripheral or central paresis, and reduced sensibility. A previous study on patients with non-terror-related multiple injuries has reported similar results (36), where acute injury-severity of gunshots did not predict 60 patients’ SF-36 scores 8 months after discharge. The authors suggested that the anatomical region of the injury (particularly central nervous system (CNS) and extremity injuries) is more predictive of long-term outcome than initial life-threatening lesions. Twelve participants reported clinically significant pain, of which healthcare needs concerning the pain condition was identified for 10 of these (e.g. neuropathic pain). The positive correlation between mean pain last week and PTS symptoms is in concordance with previous publications (37), and supports the need for a comprehensive approach for those with both psychological and physical trauma.
Several studies have reported a significant association between PTS symptoms and impaired physical health. Bugge et al. (13) reported that PTS symptoms might play a role in the development of somatic complaints among non-hospitalized injured trauma survivors, but also found that both hospitalized and non-hospitalized injured participants reported significantly higher levels of somatic complaints than the uninjured population.
The self-reported concentration and memory difficulties probably reflected the high levels of psychological and physical symptom load (including pain and sleep problems), as neuropsychological test measures were normal. Similar findings have been reported previously (38), in that no significant associations between subjective perception of cognitive difficulties and objective test measures were seen in Utøya survivors.
A major aim of healthcare services is to restore damaged body structures and functions and to prevent or limit difficulties in performing activities and roles within the context of an individual’s environment (39). We found that most of the unmet healthcare needs were related to somatic health, which might indicate that the main priority of the outreach programme (to alleviate mental health issues) did not adequately meet the needs of injured persons with somatic health issues (9, 10). A survey of the Utøya survivor population (9) identified several who had not been reached as planned. In addition to the causes discussed by Dyb et al. (e.g. non-Norwegian origin, high level of exposure and post-traumatic stress, depression/anxiety), a lack of coordinated efforts in addressing injury-related somatic illnesses, such as pain and physical restrictions, could have contributed. In accordance with this, Dyb et al. (9) found that the hospitalized participants had been contacted by their local health services less often than individuals who had not been hospitalized. Since our study recruited a majority of those with short stays at the acute hospital, this might reflect that those with short hospital stays and/or transfers to their local hospitals were at risk of reduced follow-up. In the current study, data collection was performed in an outpatient setting, and healthcare needs were based on a clinical decision process from experienced rehabilitation professionals, while the study by Stene et al. (11) recorded the survivors’ subjective opinions.
Since the physical functioning and somatic health problems were heterogeneous, the results of the current study regarding healthcare needs might reflect the importance of considering even minor physical trauma as potentially complex due to the stressful conditions under which it was obtained, and thereby the multitude of factors determining functional outcome. O’Donnell et al. (40) found that the development and maintenance of disability occurs via a complex interaction of physical factors, pain, and psychological symptoms over time. These authors concluded that, while physical and painful consequences of injury contribute significantly to long-term disability after injury, psychological symptoms play a larger role. In light of increasing awareness of the adverse physical health effects of chronic stress (35), both previous publications and our results highlight the need to address somatic health in terror survivors.
In our sample, more participants reported unsatisfactory physical than psychological health. An obvious explanation is that all the individuals had been physically injured and several were physically restricted. The current study also found an association between SF-36 PF and LSS physical and psychological health. The authors of the life satisfaction outcome used in this study suggested that life satisfaction should be defined as “reaching your own goals” (34). Our finding of unsatisfactory physical health might be explained by the expectation of having long-standing psychological symptoms, but not physical complaints, after being a victim of terror. In addition, our results of PF-SF 36 and LSS seem to be comparable to the results of Li et al. and Gao et al., who studied people who were physically injured by the 2008 Sichuan earthquake (14, 15).
Some limitations of this study require consideration. The study approvals did not allow us to compare responders and non-responders. Due to the study design and sample size, only descriptive statistics and some exploratory analyses were conducted, leaving the study exploratory. However, the study design and the integrated research and clinical practice setting allowed for a thorough clinical examination and a detailed description of health characteristics, functioning, and healthcare needs. The response rate is a strength of the current study, and the registration of injury characteristics was highly structured and well-documented. The integrated research and clinical practice setting might have biased the results by recruiting those with the most health problems. Because the study population consisted of victims of gunshot and bomb explosion, which are the most common causes of trauma after terror attacks (4, 5), we assume that the health conditions described herein reflect the traumas that occur after terror attacks in general. However, the external validity of this study might be restricted to countries with universal healthcare coverage and similar levels of health services.
This study demonstrates that many hospitalized persons following a terror attack need long-term follow-up, both for their physical and their psychological health. The hospitalized individuals reported more unsatisfying physical than psychological health, highlighting the need to address physical health issues in populations being injured under traumatic psychological circumstances. Since terror attacks account for increasing numbers of disability also in Europe, this study is considered relevant to the field of medical rehabilitation in Europe.
The authors would like to thank all participants, collaborators at the Norwegian Centre for Violence and Traumatic Stress Studies (NKVTS), Vestre Viken Hospital trust and Oslo University Hospital. Particular thanks are extended to Thomas Glott and Gro E. Paulsboe at Sunnaas Rehabilitation hospital and to Knut Magne Kolstadbråten and Nada Andelic at OUHU.
This study has been funded by the institutions noted in affiliations, and by The South-Eastern Norway Regional Health Authority.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize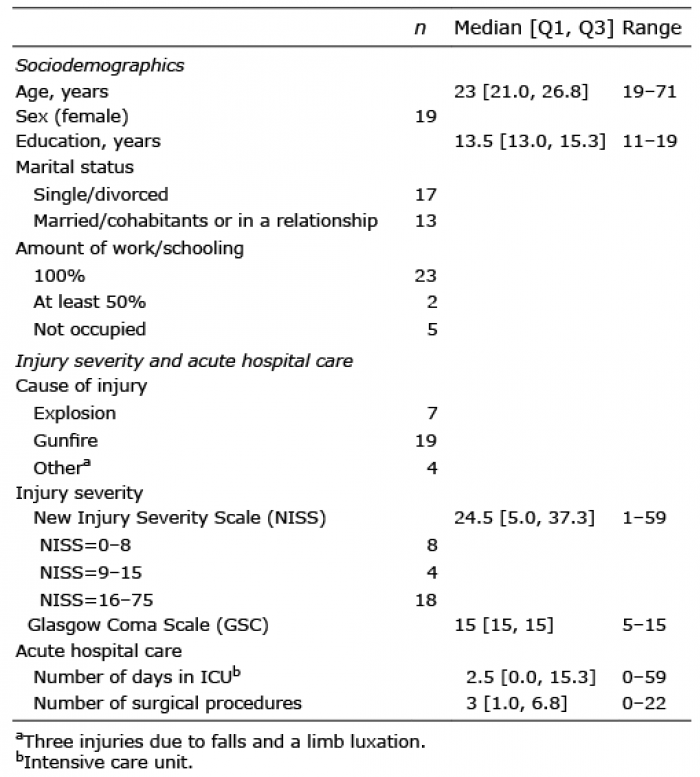 Click to show fullsize
Click to show fullsize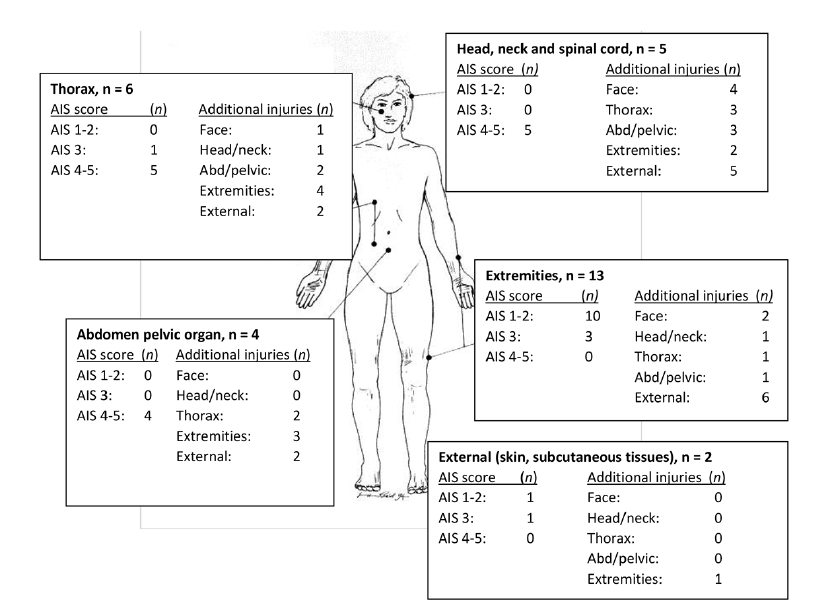 Click to show fullsize
Click to show fullsize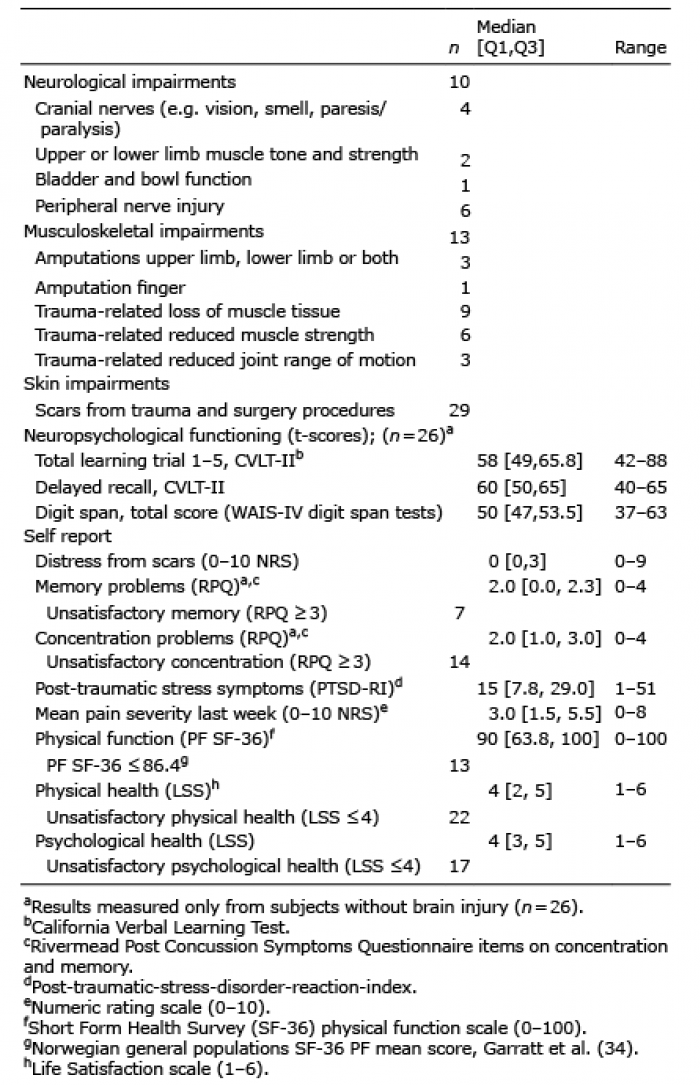 Click to show fullsize
Click to show fullsize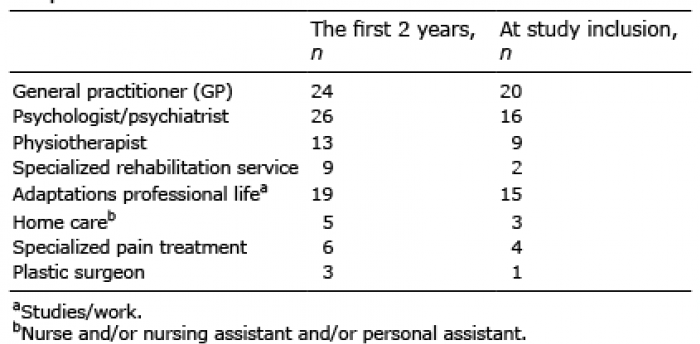 Click to show fullsize
Click to show fullsize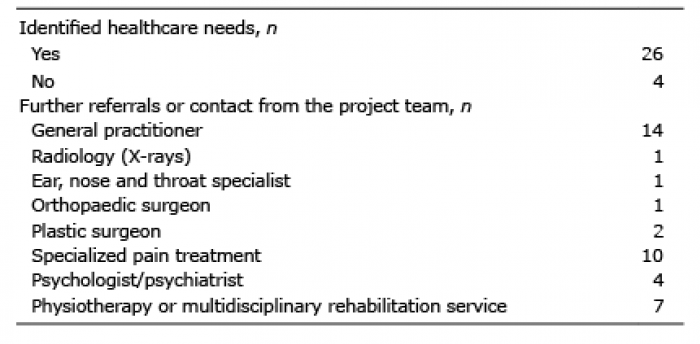 Click to show fullsize
Click to show fullsize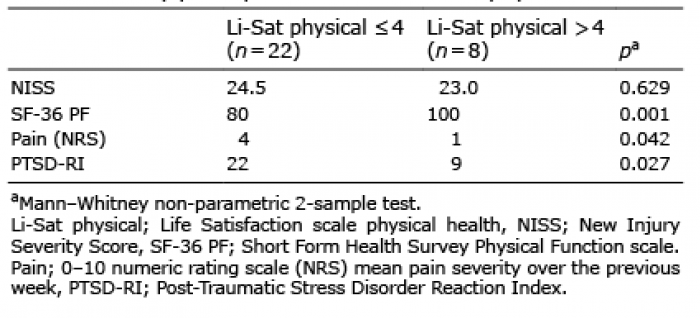 Click to show fullsize
Click to show fullsize